
A paper published in March 2026 in the journal Neuroscience is one of the more conceptually significant things I’ve read on eating disorders in a while. Written by researchers at University College Cork — a group that has been at the leading edge of gut-brain axis research — it proposes a framework that I think deserves wider attention, both for clinicians and for anyone personally navigating a complicated relationship with food.
What the paper argues
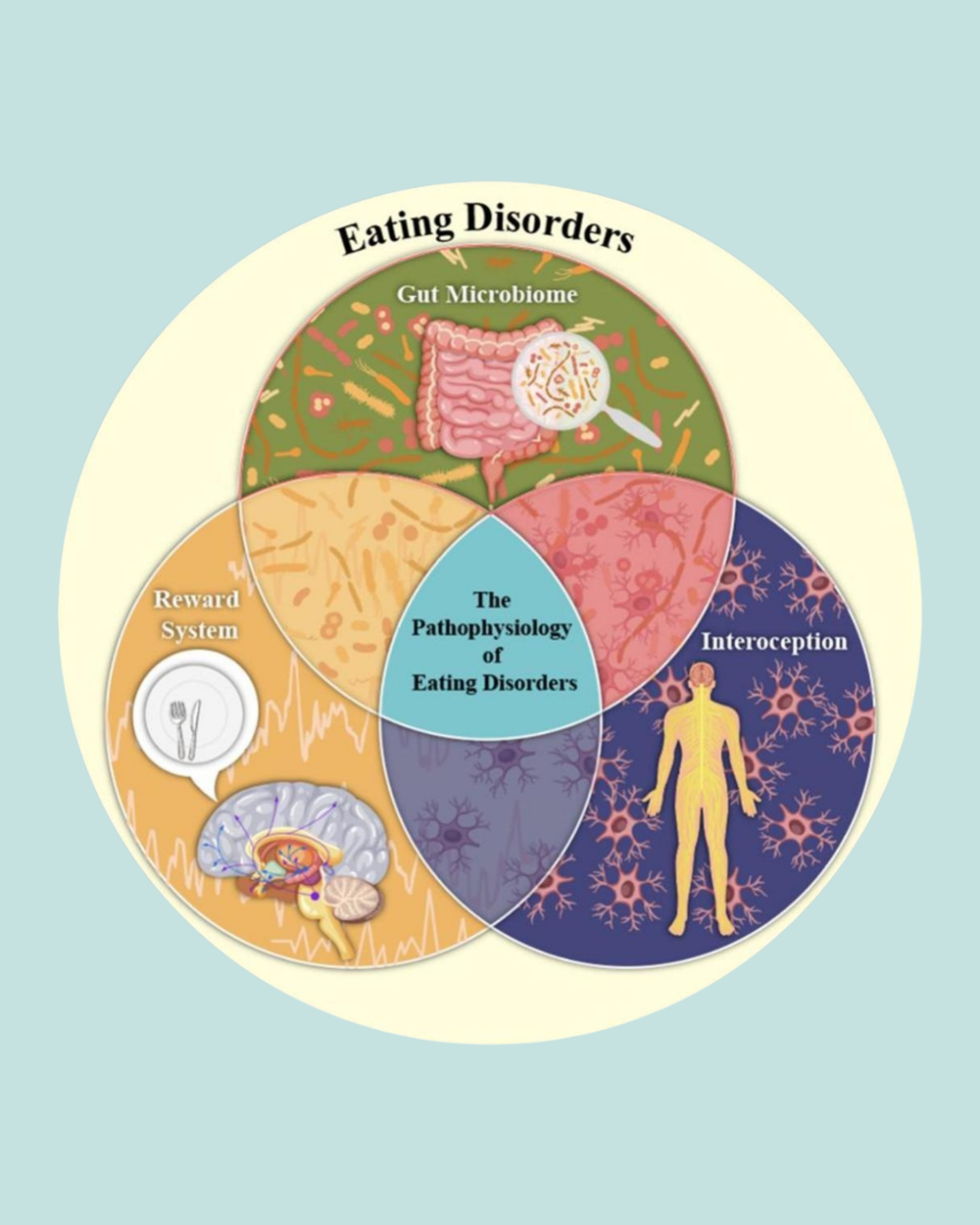
The researchers propose that eating disorders aren’t primarily neurobehavioral conditions — meaning they can’t be fully explained by thoughts, beliefs, or behavioral patterns alone. Instead, they posit a three-way biological disruption involving the gut microbiome, the brain’s reward system, and interoception.
Interoception, for those less familiar, is the body’s capacity to sense its own internal physiological states — hunger, fullness, satiety, safety, discomfort. It’s the biological infrastructure beneath what we often describe in somatic work as “body awareness” or “listening to your body.”
The researchers argue that these three systems — gut microbiome, reward circuitry, and interoceptive signaling — interact dynamically, and that disruption in any one of them tends to ripple through the others. Critically, they frame this as a transdiagnostic model, meaning it applies across eating disorder subtypes rather than being specific to anorexia or binge eating disorder alone.
What this means for overeating and sugar addiction specifically
For those who experience binge eating, compulsive overeating, or what’s often described as sugar or food addiction, this framework is particularly relevant.
When the gut microbiome is dysregulated — through chronic stress, dietary restriction, antibiotic use, or ultra-processed food consumption — it disrupts dopamine signaling in the brain’s reward regions. The practical result: food becomes less satisfying, the “I’ve had enough” signal is blunted or delayed, incentive salience (the pull toward food) increases, and cravings intensify. This is not a character flaw or a lack of discipline. It’s a measurable biological dysregulation.
Simultaneously, interoceptive impairment means the hunger and fullness signals that should guide eating behavior become unreliable. People may genuinely not feel satiety until well past the point of physical fullness, or may experience hunger signals as anxiety rather than recognizing them as hunger. These aren’t psychological distortions in the traditional sense — they’re disruptions in the body’s sensory feedback systems.
My initial reaction — and why the psychological piece still matters
My first response reading this paper was the same question I’d expect from most practitioners working in this space: what about psychology? What about the role of trauma, early relational experiences, and the ways food becomes a coping strategy when the nervous system has no other resource?
The paper acknowledges the broader biopsychosocial context — mentioning genetic vulnerability, comorbid mental health conditions, and chronic stress as part of the etiological picture. But it doesn’t genuinely integrate the psychological layer into its proposed framework. The trauma piece is bracketed rather than woven in.
This is a real limitation. And I want to address it — not to critique the paper, which is doing something valuable within its scope, but because I think the integration matters enormously for how we apply these ideas clinically.
Where the frameworks converge
Here is what I find most compelling: the biological framework proposed in this paper and the trauma-informed, somatic psychological framework are not in conflict. They may be describing the same underlying process at different levels of analysis.
Chronic early stress and adverse childhood experiences dysregulate the HPA axis — the body’s central stress response system. That dysregulation alters gut microbiome composition. It changes dopamine signaling in reward regions. It impairs interoceptive accuracy and vagal tone. The biological disruptions this paper documents — the microbiome dysbiosis, the reward processing alterations, the interoceptive deficits — may be the downstream physiological expression of the psychological histories that so many people with eating disorders carry.
The child who learned to disconnect from bodily sensation in order to survive an unpredictable or unsafe environment becomes the adult with measurably altered vagal tone, dysregulated interoceptive signaling, and a gut-brain axis that has been shaped by years of chronic stress. The nervous system adaptations that were once protective become the substrate for disordered eating in adult life.
The paper actually gestures toward this connection — noting that early life adversity has been linked to visceral hypersensitivity and lasting alterations in gut-brain responses. But it stops short of connecting those dots back to attachment, coping, and the psychological function that eating behaviors serve.
Practical implications
What this framework offers is a set of biological intervention targets that can work alongside somatic and trauma-informed approaches rather than replacing them. Microbiome-targeted interventions — including specific probiotic strains, prebiotics, and dietary approaches — may support the gut-brain signaling that underpins reward regulation and interoceptive accuracy. Vagus nerve stimulation, both through devices and through somatic practices that increase vagal tone, directly addresses the interoceptive pathway. These aren’t replacements for the psychological work. They’re biological supports that may make that work more accessible and sustainable.
For practitioners, this is an invitation to think in layers: the psychological history that shaped the nervous system, the somatic patterns that express it, and the biological environment — particularly the gut-brain axis — that either supports or undermines recovery.
For anyone personally navigating this: your body is not broken and your relationship with food is not a moral failure. It is a system that learned to adapt, and that adaptation has biological depth. That also means healing has biological depth — and more levers to pull than most conventional treatment approaches have acknowledged.
The paper is open access: Ziade, McDermott, O’Riordan, Cryan & Schneider, Neuroscience, Vol. 603, 2026.